Here's a thread about a paper I recently read that...
Length: • 6 mins
Annotated by Nick
Here's a thread about a paper I recently read that made me genuinely *furious*.
It's a paper from 1980.
You know... 40 years before the pandemic began.
You wanna know the title?
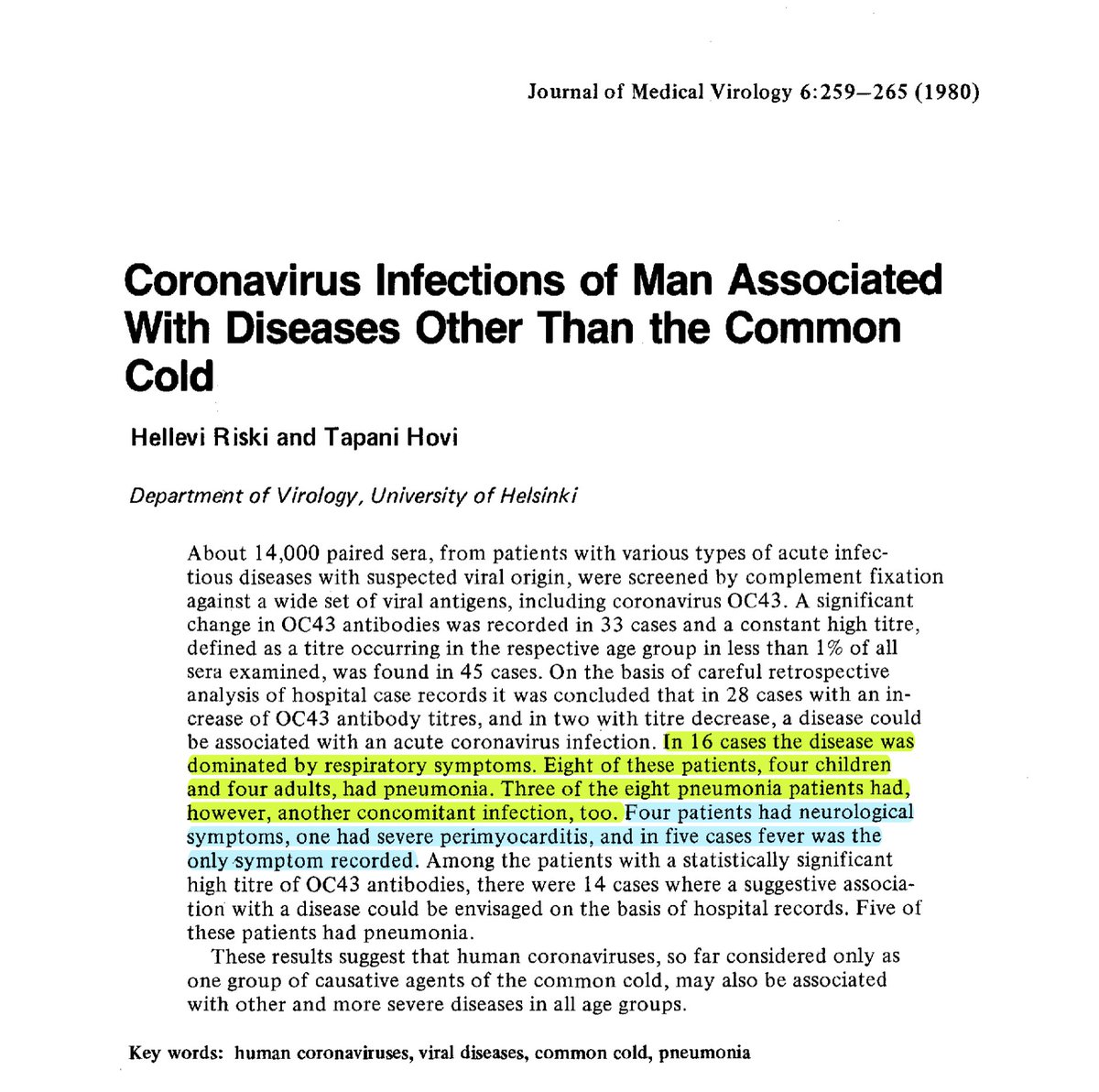
"Coronavirus Infections of Man Associated With Diseases Other Than the Common Cold"
1/
If you're now thinking "well, it probably can also cause pneumonia and acute respiratory distress syndrome," you'd be correct. If you guessed another major LC issue, neurological symptoms, YOU'RE CORRECT AGAIN.
But it gets worse! Let's take a little tour of the method...
2/
It had a small number of participants drawn from a HUGE pool:
14,000 paired sera samples (1 pair=1 person, 2 time points) were screened for changes in HCoV-OC43 antibodies
Significant changes found in 33 cases
Constant high titers in 45 cases
78 cases total
3/
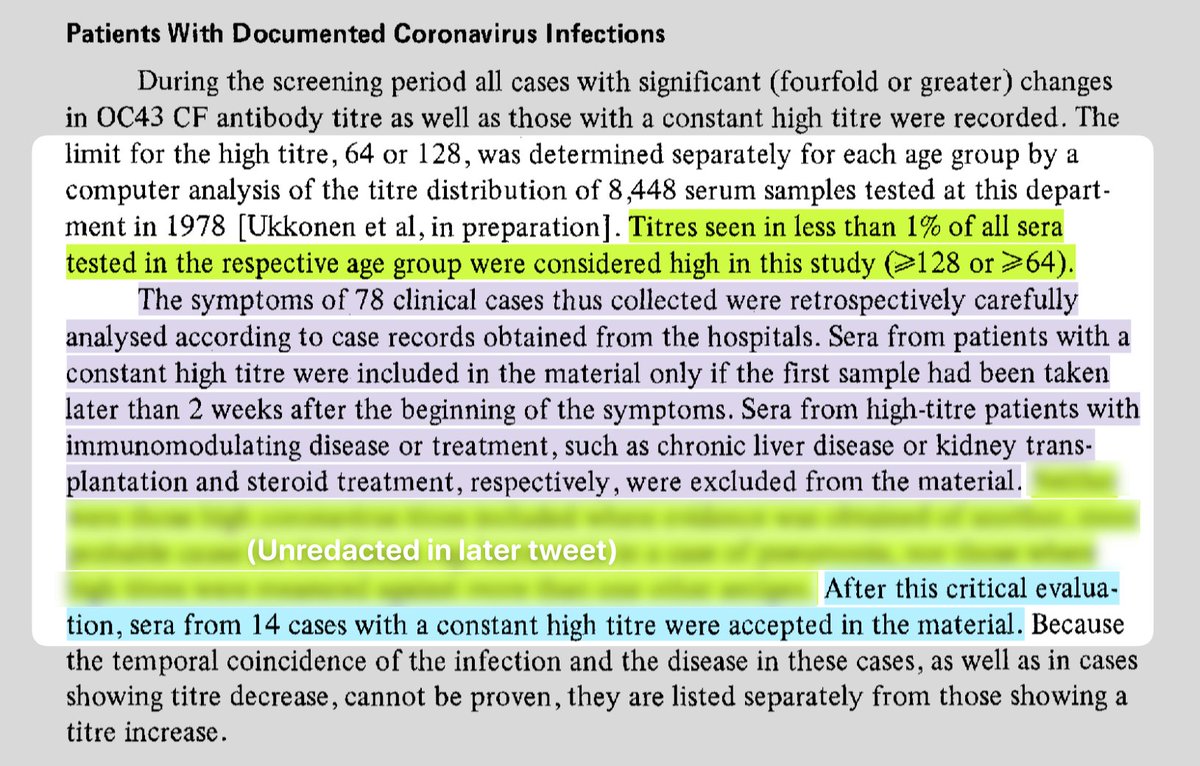
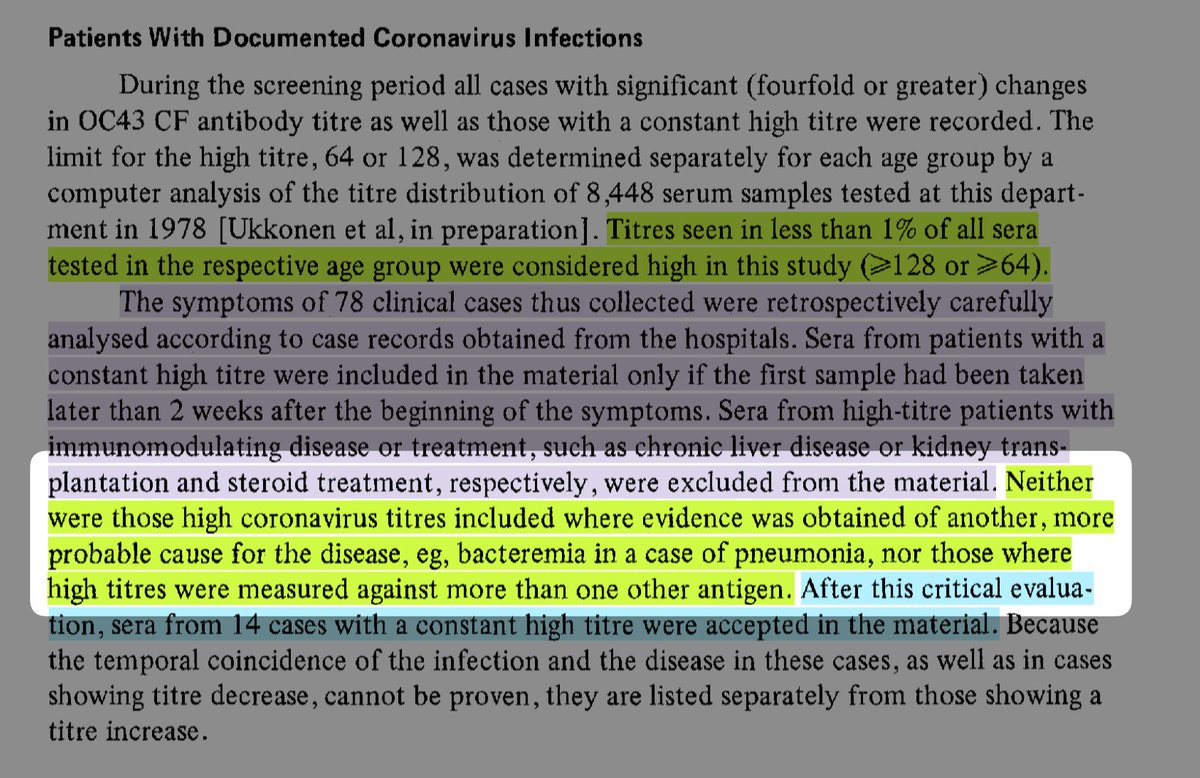
Selection criteria ensured only cases most *directly* related to OC43 are included:
"High" titers value is in less than 1% of cases from another study
Exclude existing immune issues
Exclude constant-high titers taken <2 weeks apart
Keep decreases separate
4/
If you're thinking that these results aren't *super* notable, because any virus has the possibility of rare, dangerous complications, hold that thought, because that's the beauty of the selection criteria.
These cases aren't a collection of the most *severe* outcomes...
5/
These are the samples from a cohort of 14,000 for which the documented symptoms could be DIRECTLY ASSOCIATED with measured OC43 antibodies.
That is, the criteria are explicitly designed to eliminate every confounding variable known at the time.
6/
There are two critical criteria that make these results significant (and IMO, robust):
- Cases excluded when there was another probable (non-coronavirus) cause in the patient's medical record
- Cases were excluded when high titers were measured against multiple other antigens
7/
Overall, the cases examined in this study—out of 14,000 samples—are ONLY those
with symptoms documented in the medical record,
that fall between the time the samples in each pair were taken, and
that are UNLIKELY to have been caused by any other condition.
8/
To put it another way, the cases that were included in the study are those for which:
HCoV-OC43 is the most probable cause of the symptoms
every patient was very likely to be considered *generally healthy* before they were infected with OC43
9/
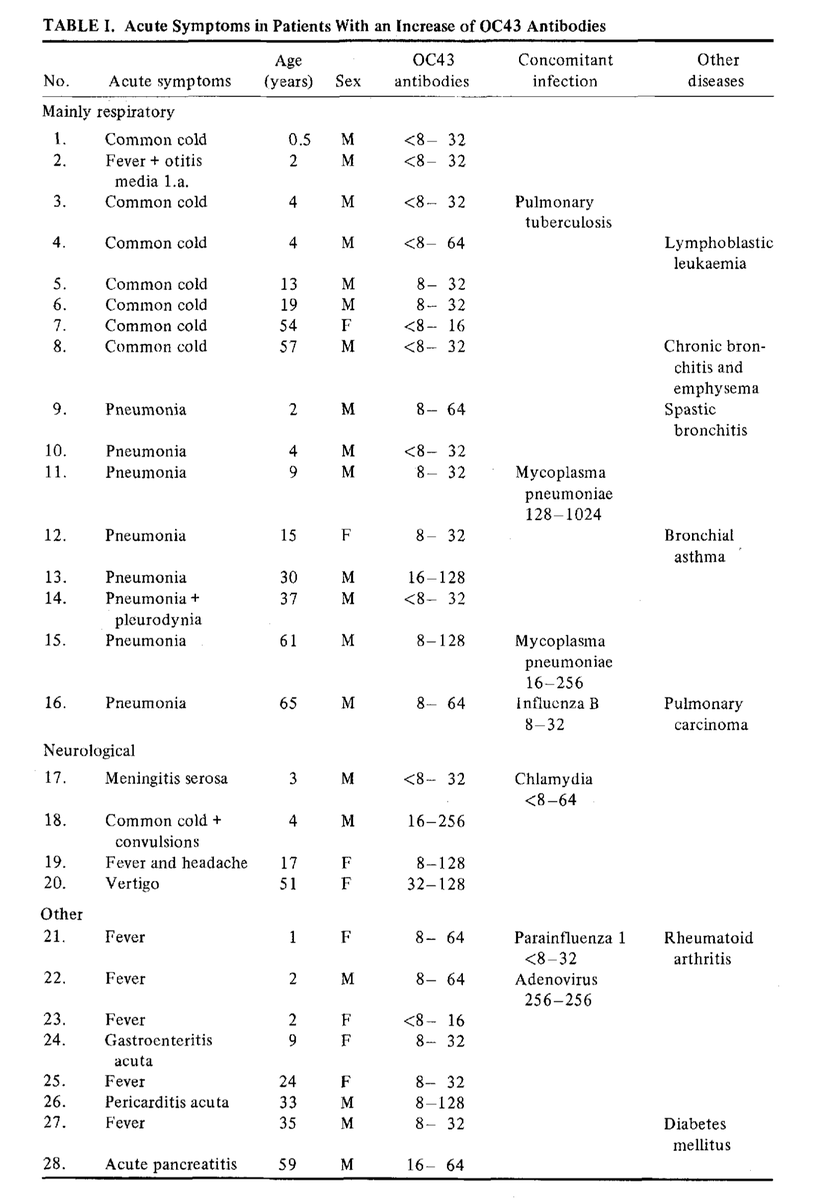
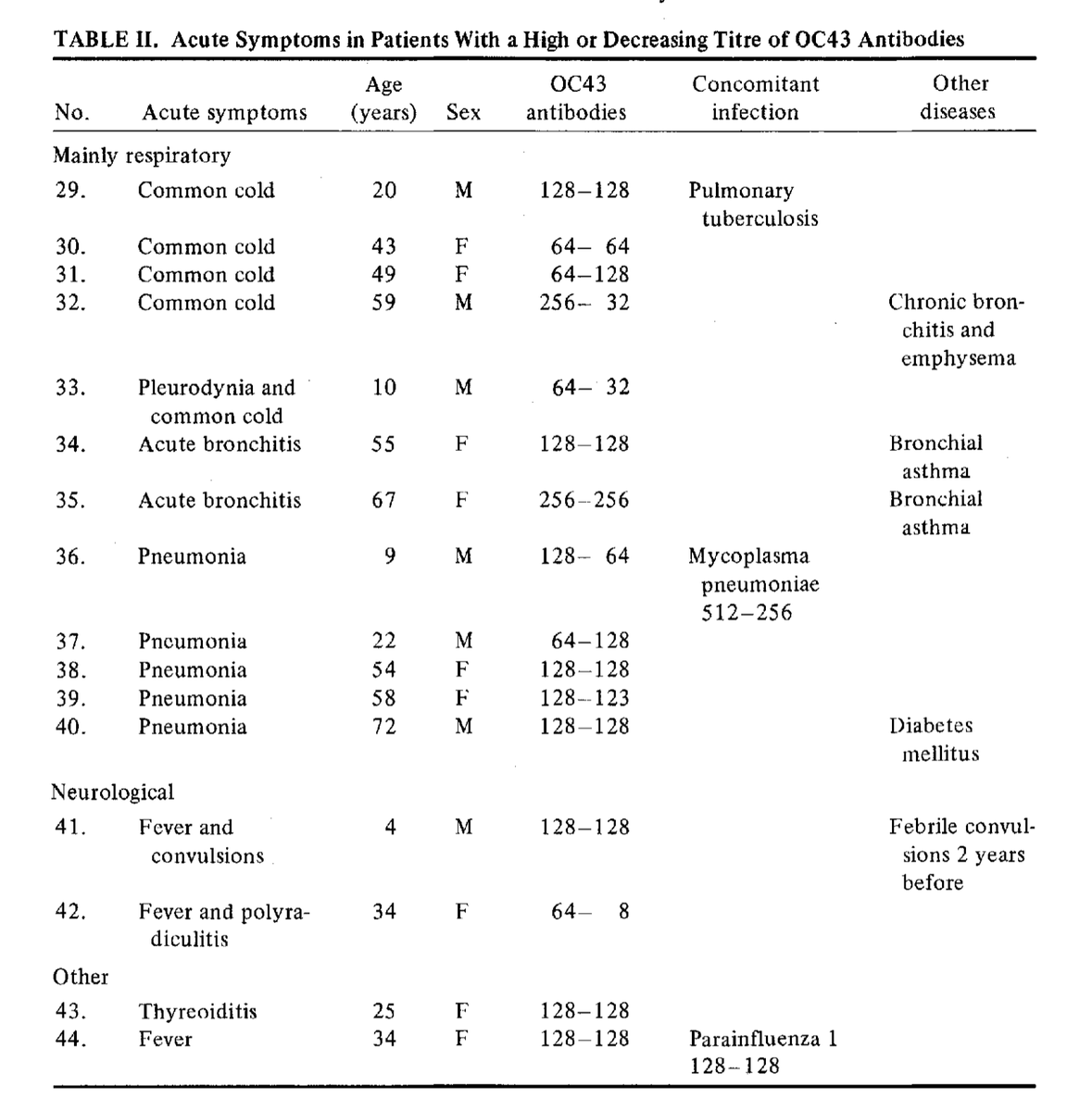
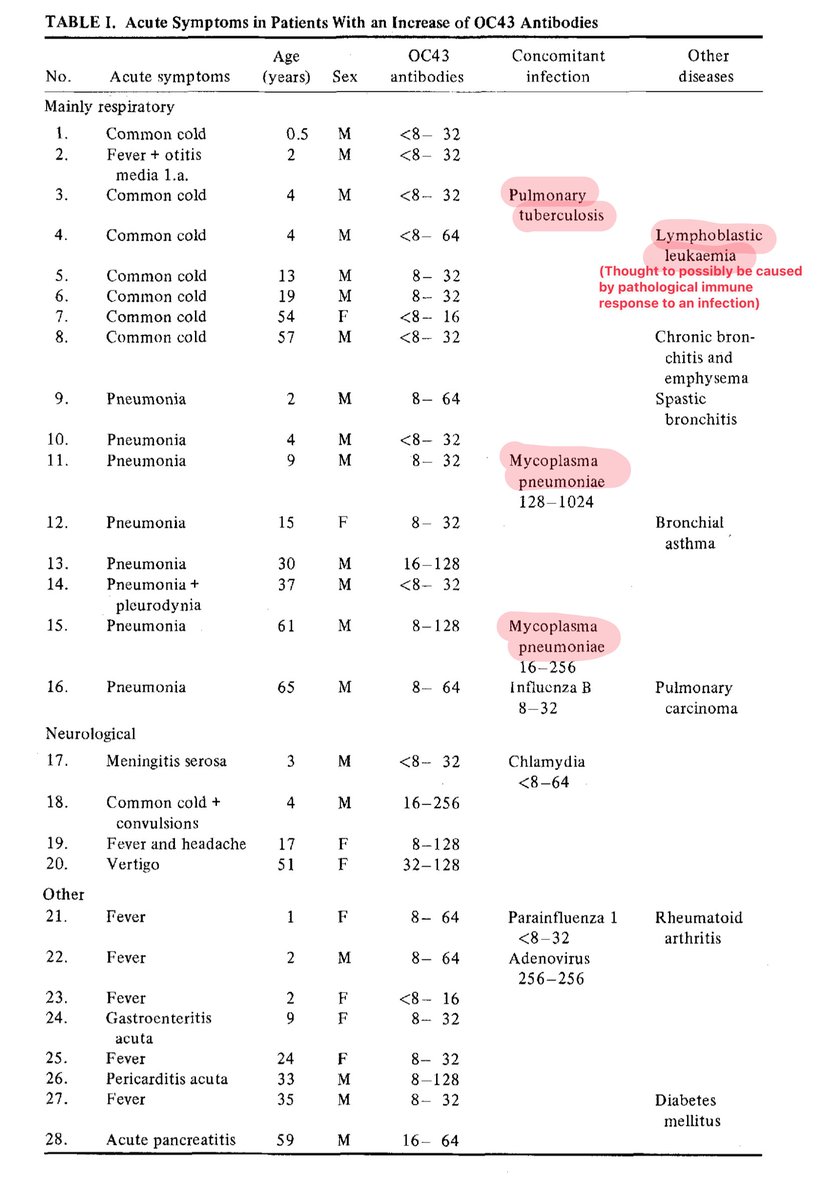
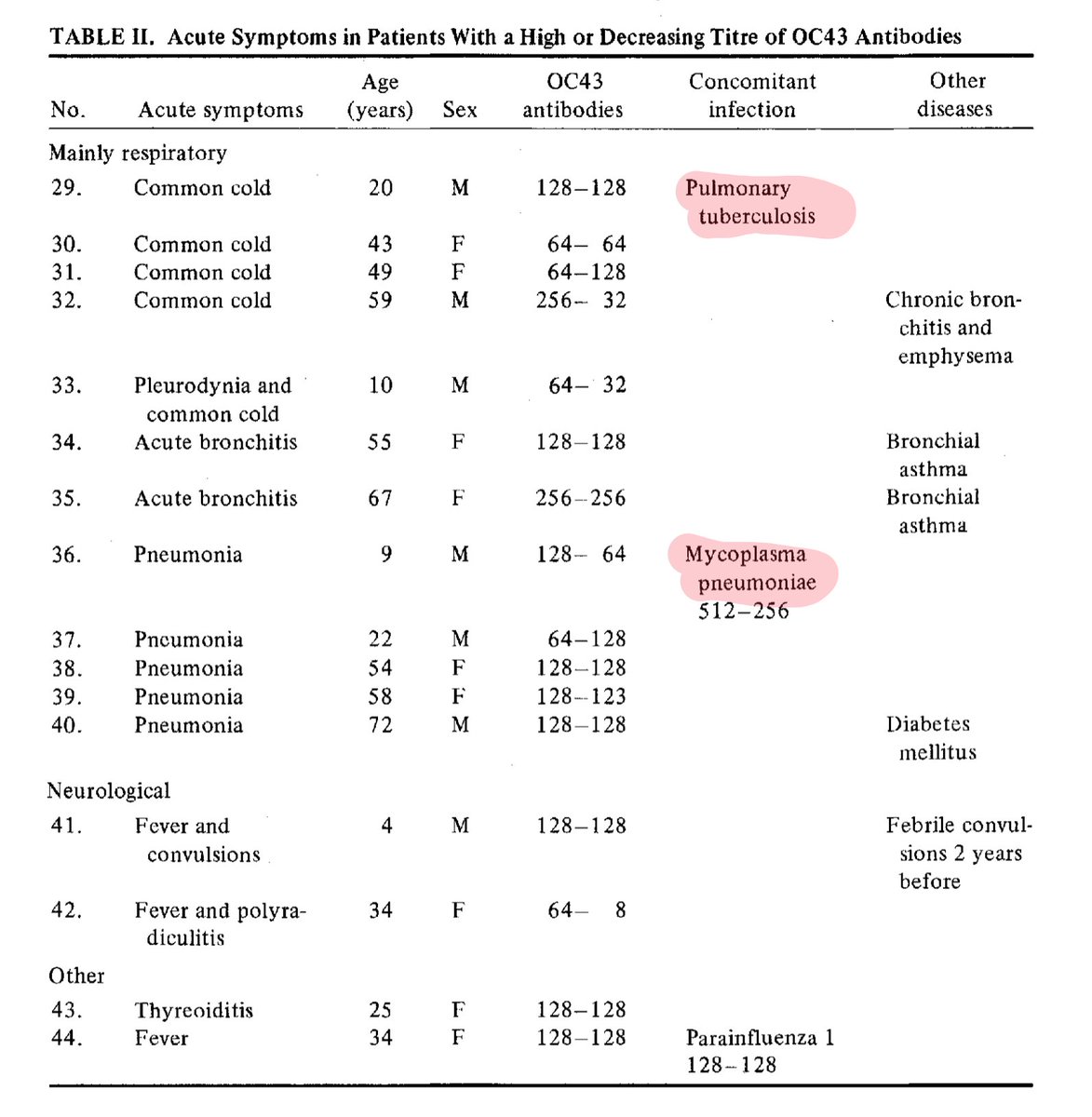
These strict criteria leave us with just 28 patients who had an increase of OC43 antibodies, and just 16 who had a constant-high or decreasing titer of OC43 antibodies, 44 in total.
4/28 (14%) and 2/16 (12%) had neurological symptoms.
Their ages were 3, 4, 4, 17, 34, 51.
10/
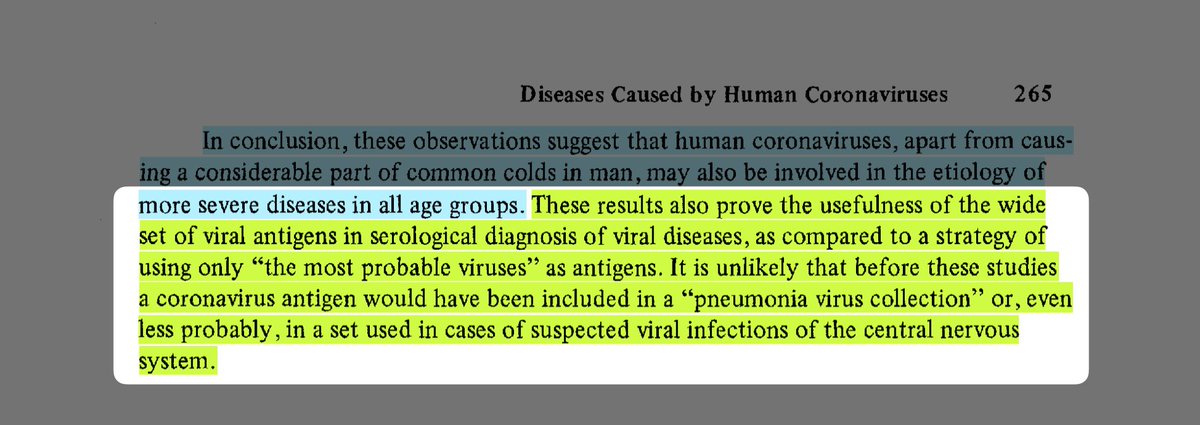
Their conclusion is clear: human coronaviruses may also be involved in OTHER severe diseases in ALL AGE GROUPS.
Remember, this was the conclusion of a serological study conducted OVER 40 YEARS AGO.
11/
All of this is even summarized concisely in the abstract!
We've known since 1980—with some degree of confidence—that human coronaviruses can cause neurological symptoms in all age groups.
Why wasn't this public knowledge in 2020????
Study link: ncbi.nlm.nih.gov/pmc/articles/P...
12/
[Everything past this point is my own interpretation!]
For reference, it was published a year before the first news story about unexpected opportunistic infections.
Two before GRID was renamed AIDS.
Three before a virus was isolated.
Six before the virus was renamed HIV.
13/
1980 had a knowledge vacuum about T-lymphotropic viruses, and immunotropic viruses in general!
In comparison, for example, we know that SARS-CoV-2 can cause immune system dysregulation and deficiency, including T-cell exhaustion! It's well-documented at this point!
14/
With this in mind, do you see any potential issues with the exclusion criteria?
IMO, in retrospect, they erred in excluding samples where high titers were found for MULTIPLE other antigens. There's a hint that this may be a confounder in the list of concomitant infections!
15/
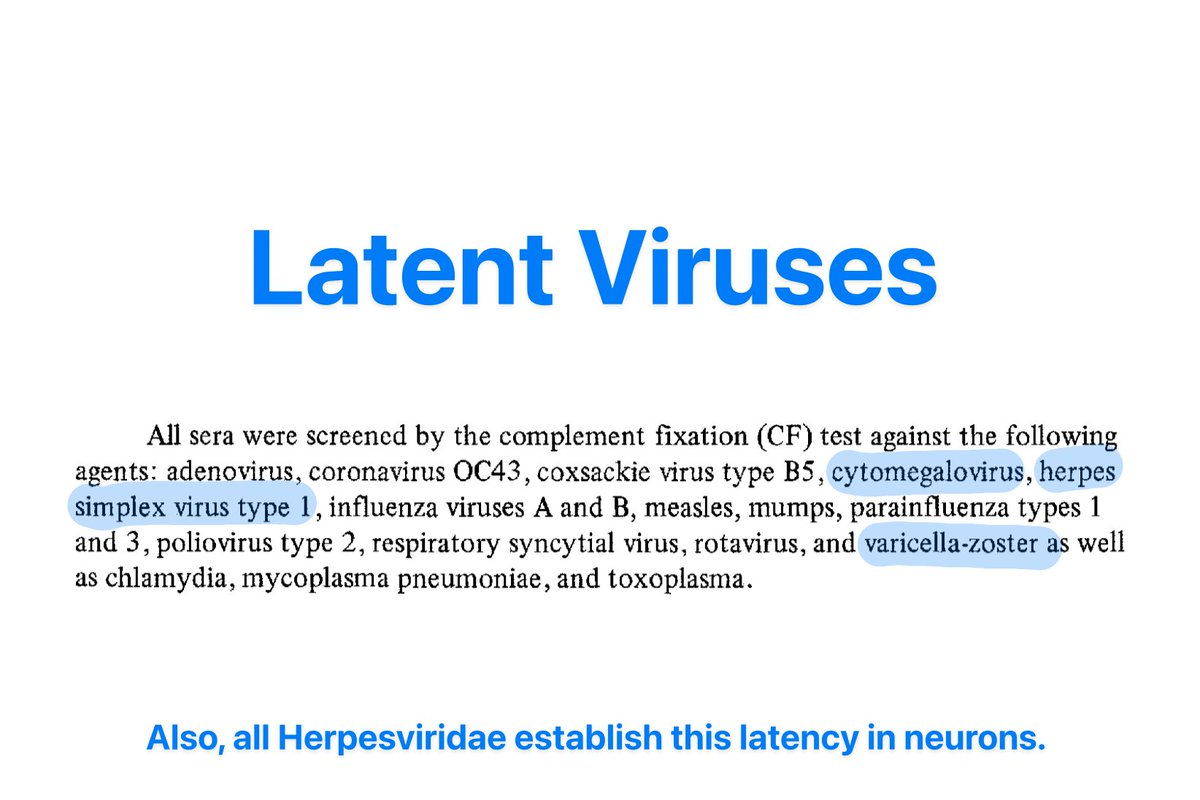
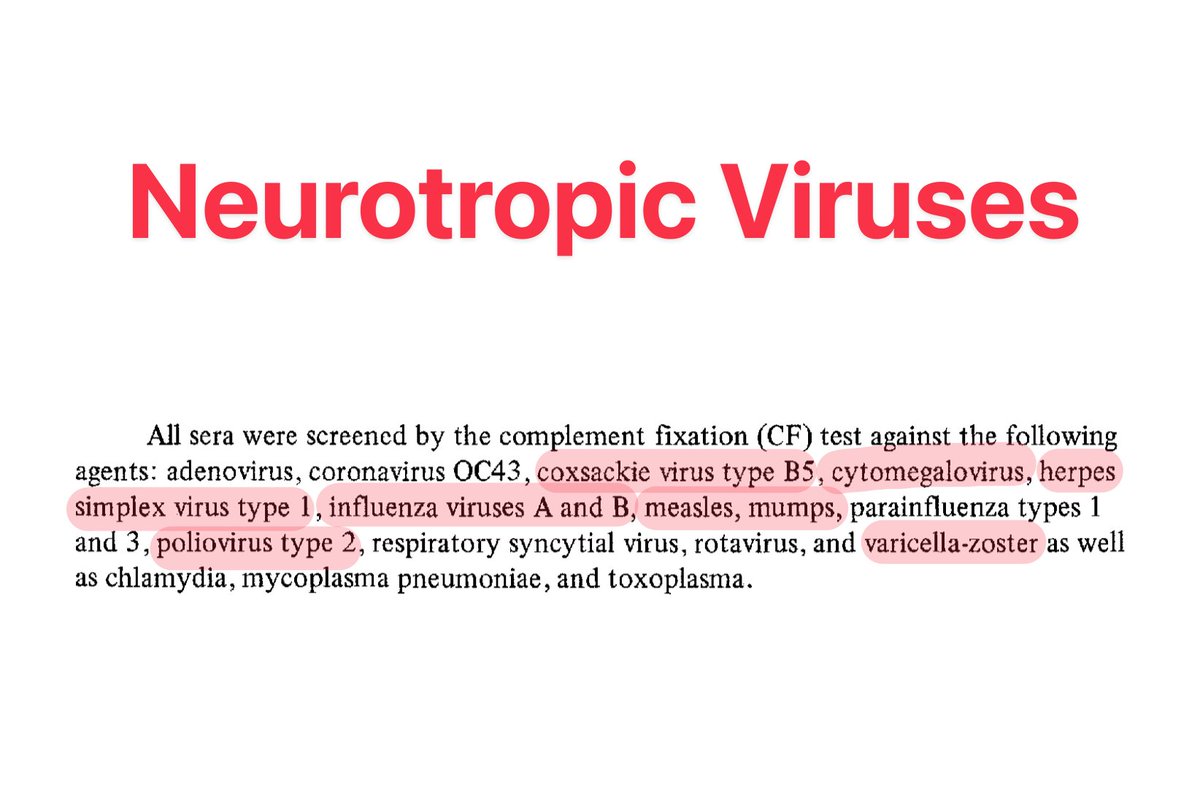
See, the list of other titers checked included a lot of viruses that are:
- NOW known to be neurotropic and/or
- NOW known to cause latent infection
16/
With the lone exception of a 65yo with pulmonary carcinoma and pneumonia who had concomitant Influenza B, NONE of the other viruses highlighted in the previous tweet are present.
There are, however, other conditions known to emerge in the presence of immune dysfunction.
17/
Reiterating the key points:
1. SARS-CoV-2 is also known to cause immunosuppression
2. Lack of concomitant neurotropic virus antibodies
3. Lack of concomitant latent virus antibodies
4. Presence of antibodies from a common opportunistic infection
18/
5. Criteria excluded those with high titers to multiple other pathogens
6. Criteria excluded those with immunomodulating disease/treatment
7. Study only looks at symptoms during acute illness
8. Criteria included only symptomatic disease exclusively associated with OC43
19/
From this, I'm concluding that, in my opinion:
12% is more likely than not to be the FLOOR for acute neurological symptoms resulting from OC43 infection
OC43 likely also causes mild immune dysregulation
20/
Surprisingly, I couldn't find much one way or the other about immune dysregulation from ANY non-SARS, non-MERS human coronavirus infection.
So... someone who can do something with this information... have a couple free hypotheses, I guess?
21/21
22/21
I noticed I describe the same thing as both robust and an error, so I feel like I should clarify: the study’s inclusion criteria were as robust as they could be based on what they knew, and they erred only in the clarity of hindsight!
23/21
I actually don’t even think some of the statistical methods they’d need to use to account for the mediating variables had been fully developed yet. Mediation models were developed in the 80s, and a lot of development of moderated mediation models is much more recent
24/21
I should add that I’ve known *of* this paper for a while, because it’s cited in a handful of reviews. However, the way it gets cited makes it sound like a case report, not a 14,000 sample serology cohort study
25/21
Just realized I said “why wasn’t this public knowledge?” when I meant to say “why wasn’t this COMMON knowledge?”
Not trying to imply that it was *hidden*, just *inadequately communicated*
26/21
This isn't exactly about the results, but is just really funny to me: I don't think this paper was written SPECIFICALLY because they had an interest in OC43.
I think they wrote this paper to (correctly) prove a point about other people's shitty methods 🤣
27/21
tl;dr 1:

These results align well with a lot of the recent covid-related studies that have been published. The proportion of people with neuro symptoms is roughly similar to what we see with covid, so public health agencies shouldn't have been surprised by the neurological symptoms!
28/21
tl;dr 2:
You are 99% correct! The only *minor* error is that the paper is about *acute* neurological symptoms (occurs DURING the infection, then gets better) rather than long-term complications.
Of course, I haven't seen anything that would lead me to believe long-OC43 doesn't occur!
29/21
tl;dr 3:
But regardless of the duration of these symptoms, the fact that the *proportions* of acute neurological symptoms and severe respiratory symptoms line up, roughly, with what we see in covid, it's extra-infuriating.
30/21
tl;dr 4:
This study puts a lot of effort into finding cases of Human Coronavirus OC43 (an older virus) that are unlikely to have other explanations. Out of the cases they found, about 12% showed symptoms in their brains and nervous systems.
31/21 There's a valid point a couple people raised that I kinda just forgot to address! Additional context worth knowing:
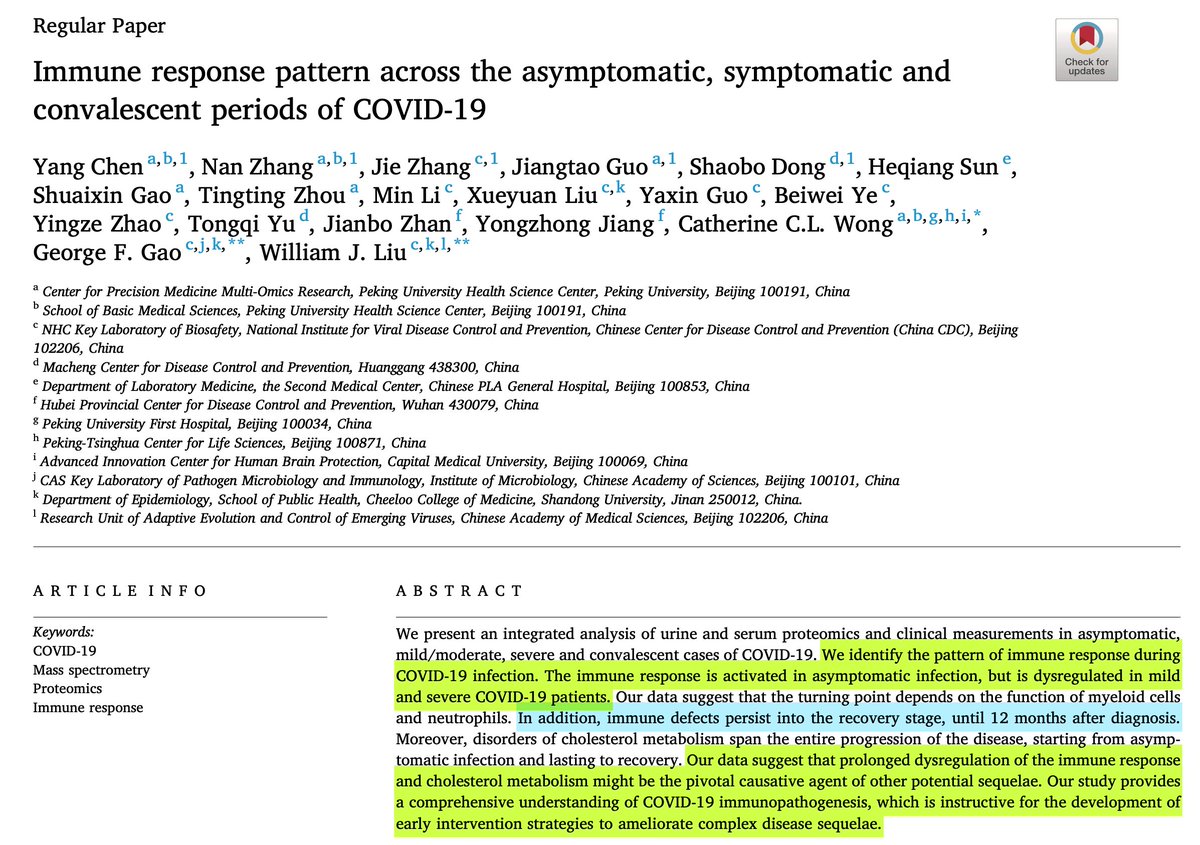
In covid, immune dysfunction has been found across MILD, MODERATE, and SEVERE acute infections, for at least 6-12 months afterward.
32/21 And a paper published last month found that covid is attacking, well, just a whole bunch of different immune cells in people with Long Covid:
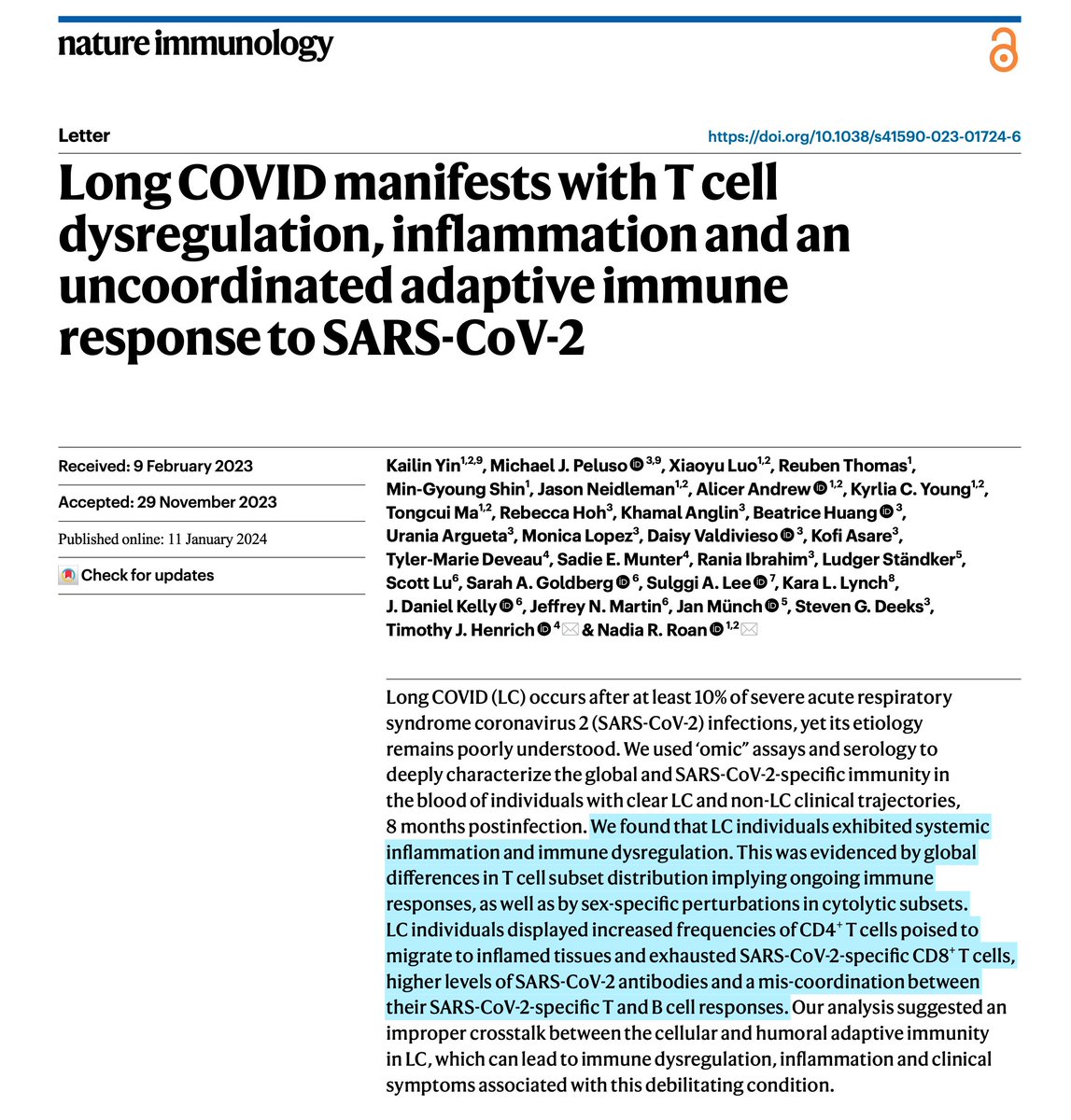
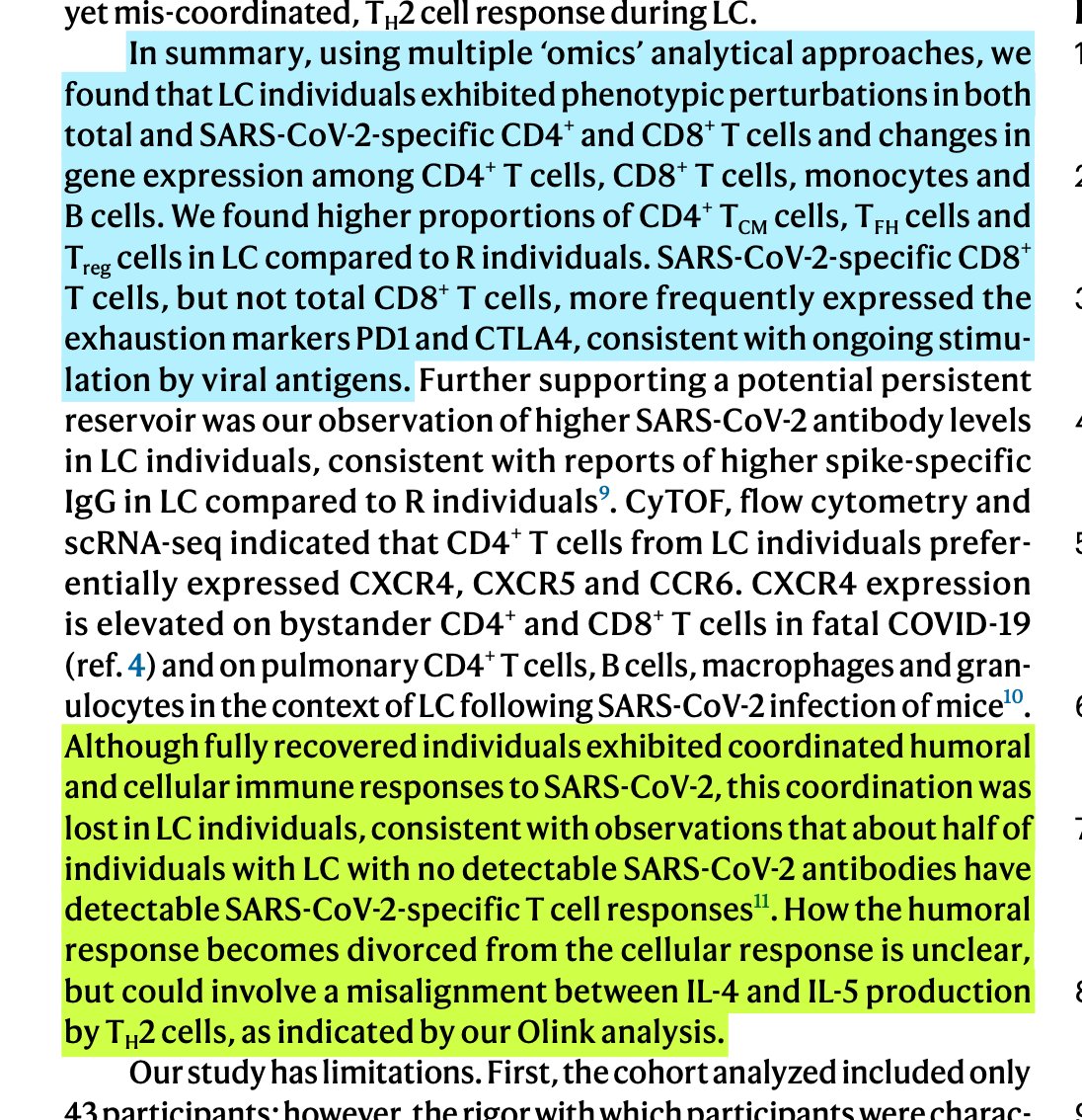
33/21 I have no idea what inference to draw from the combination of those papers. Each on its own is BAD.
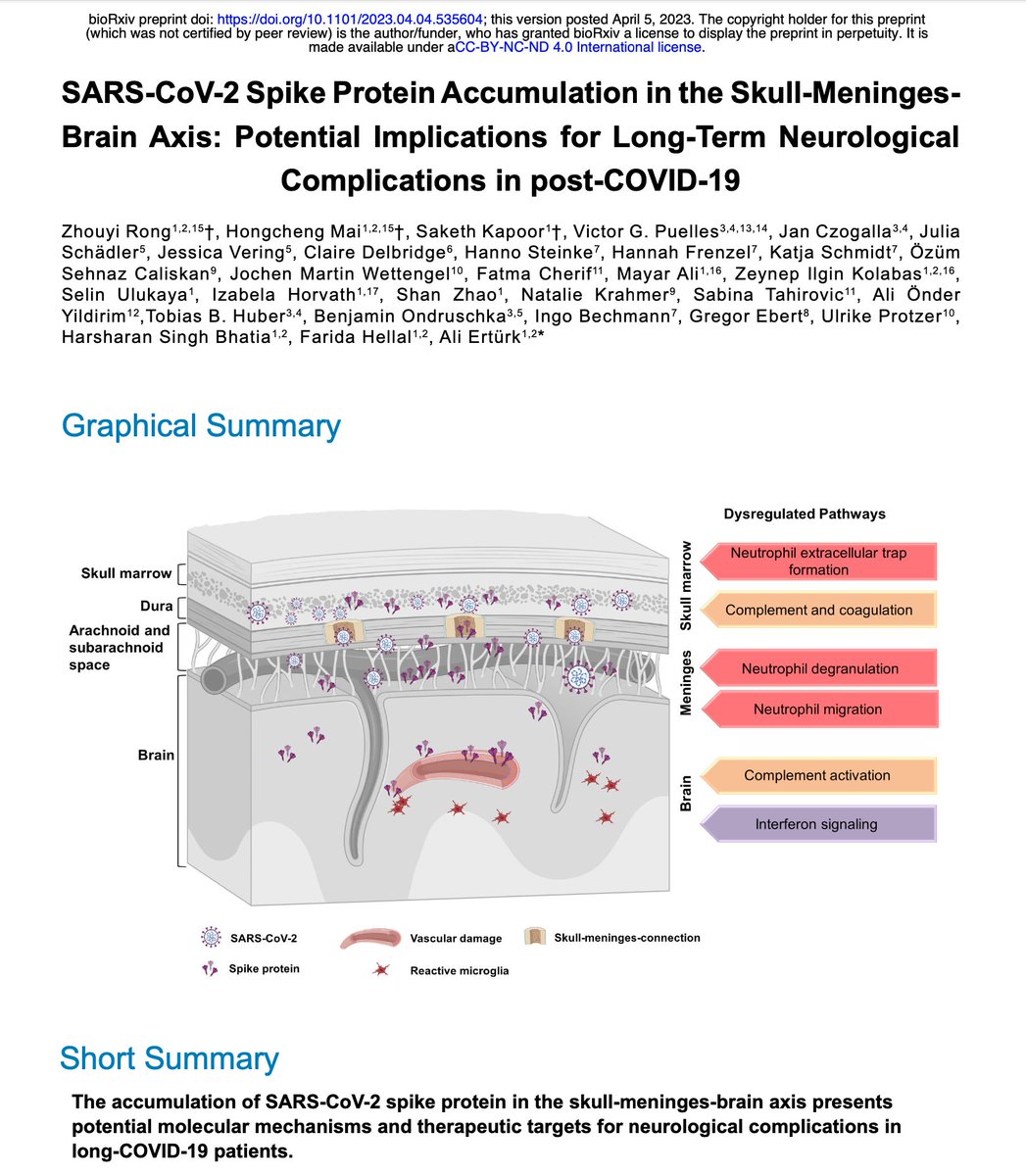
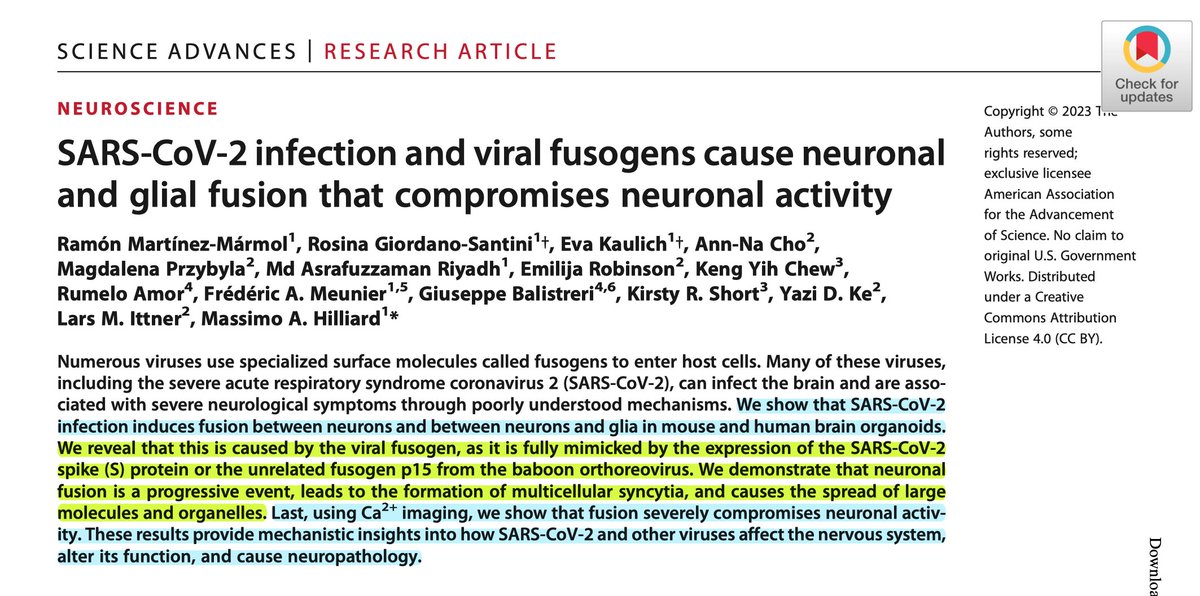
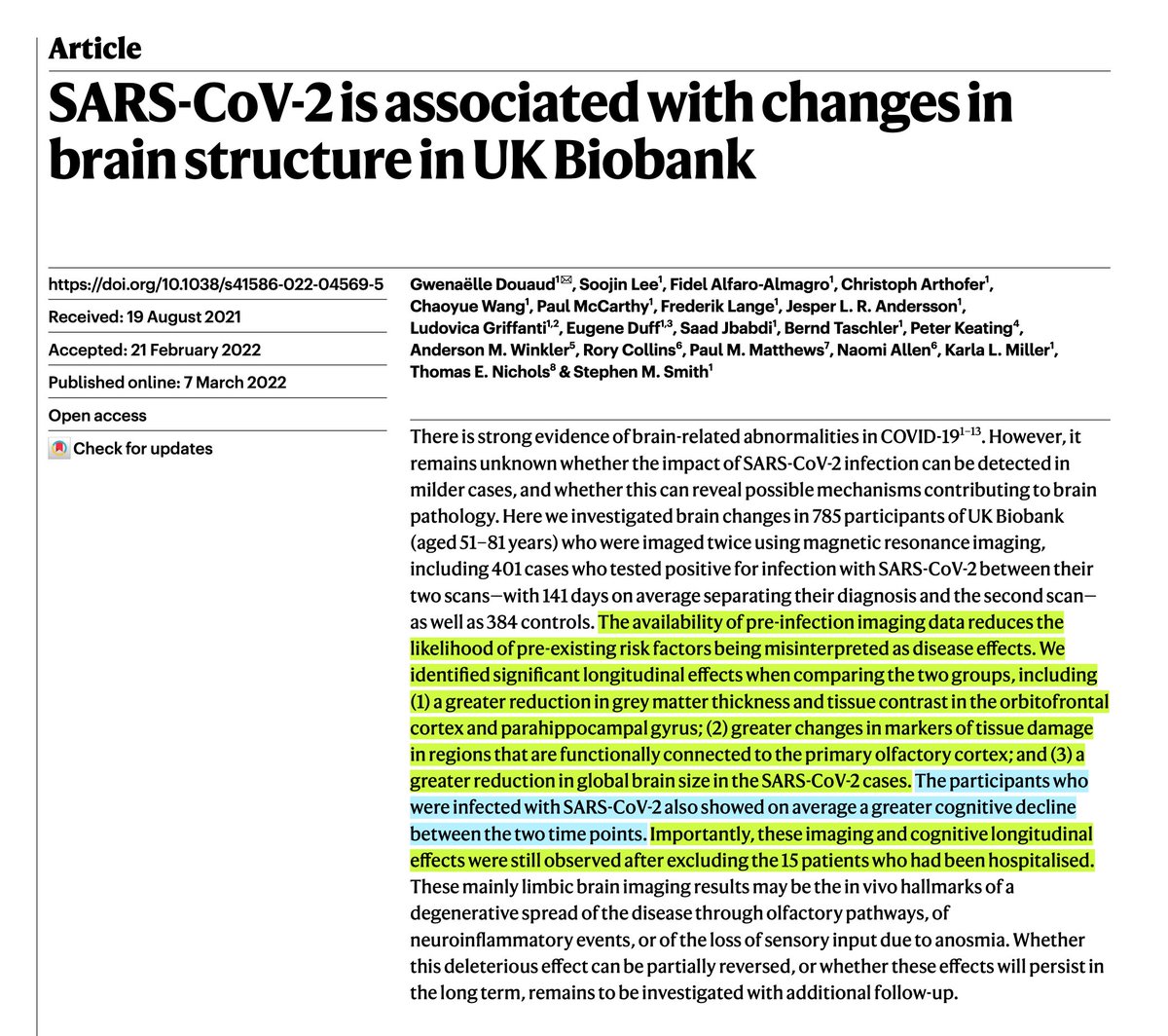
But considering SARS-CoV-2 can:
- Can get stuck in our brains
- Fuse our brain cells together
- It shrinks brains even in MILD cases
coronaviruses are tricky little shits.
34/21 Which is why I wear an N95 mask or better (also known as a "filtering facepiece respirator") in shared air, because you filter pathogens out of the air you're inhaling, you can't be infected by them!
I haven't been sick in 3 years, 8 months to the day! It's great!