Lithium's Mechanism of Action: An Illustrated Review
Length: • 4 mins
Annotated by Zakhar
Zakhar:

This tutorial discusses:
- Brain abnormalities found in patients suffering from bipolar disorder
- How lithium modulates dopamine, glutamate and GABA
- Intracellular changes associated with lithium use (effects on proteins such as PKC, MARCKS, GSK-3, IPPase and IMPase)
Some content could not be imported from the original document. View content ↗
Lithium MOA: Text Version
Unravelling the mystery of how lithium works is one of the greatest challenges psychiatry faces today. There have been significant advances in the last couple of decades, mainly in neuroimaging. This has allowed to integrate findings in brain structure to the potential mechanism of action of lithium. This diagram shows that lithium has multiple levels of action, from macroscopic to microscopic levels. In the next slides we’ll discuss some abnormalities found in brain structure of bipolar patients and changes in brain structure linked to lithium therapy. Then, we’ll study how lithium modulates dopaminergic, glutamatergic and gabaergic neurotransmission. Finally, we’ll explore intracellular changes associated with lithium use.
Some of the abnormalities found in patients with bipolar disorder involve the fronto-limbic network. This includes subcortical structures such as the hippocampus, amygdala and striatum. Some cortical regions have been implicated, these findings depend on many factors such as population studied, number of episodes and region of interest.
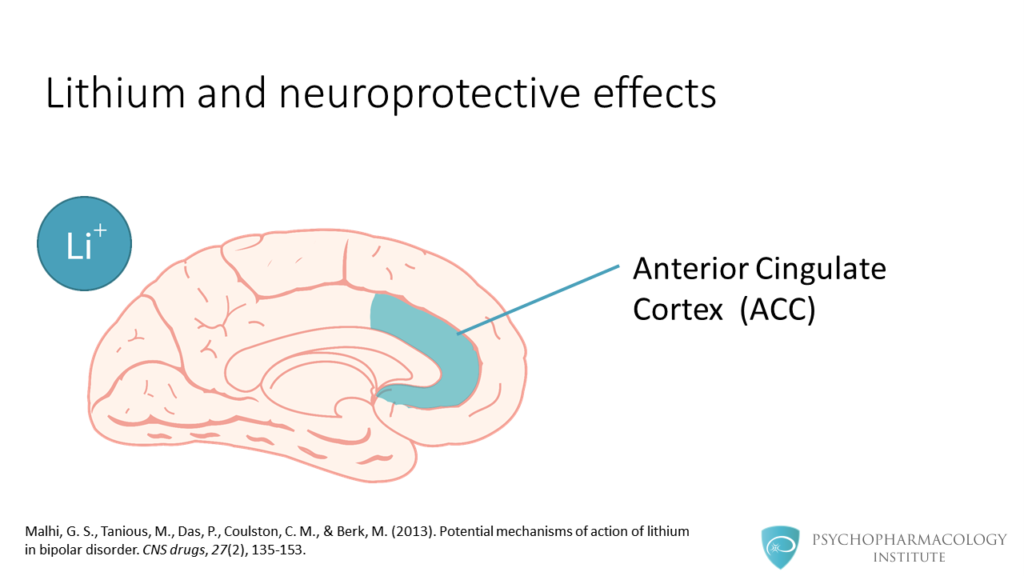
Lithium has shown neuroprotective effects in a number of brain regions. This has been suggested by changes in grey matter volume. In the next slides we’ll see regions that have shown improvement after lithium treatment. The first here is the anterior cingulate cortex.
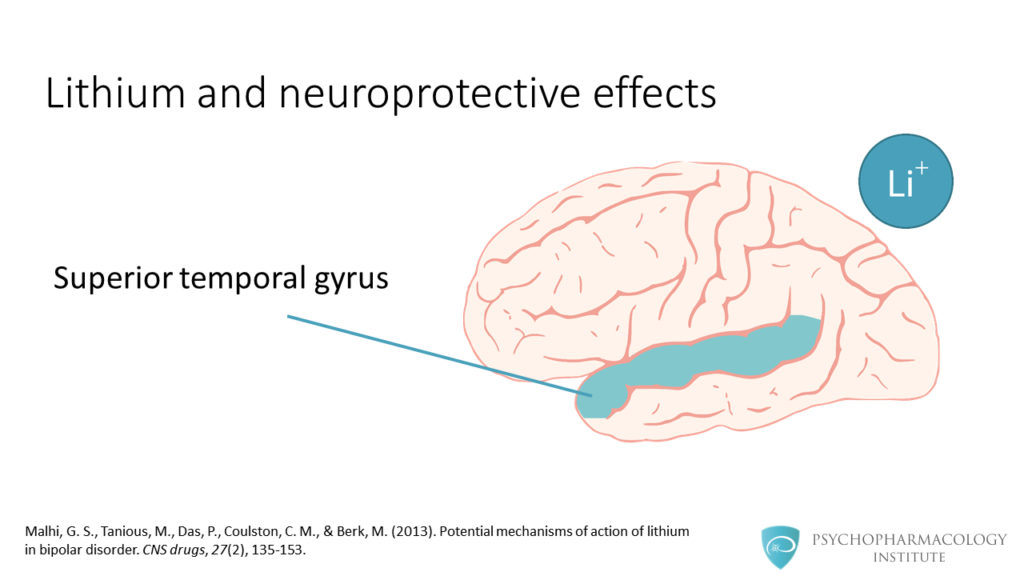
Also, studies have shown changes in the superior temporal gyrus.
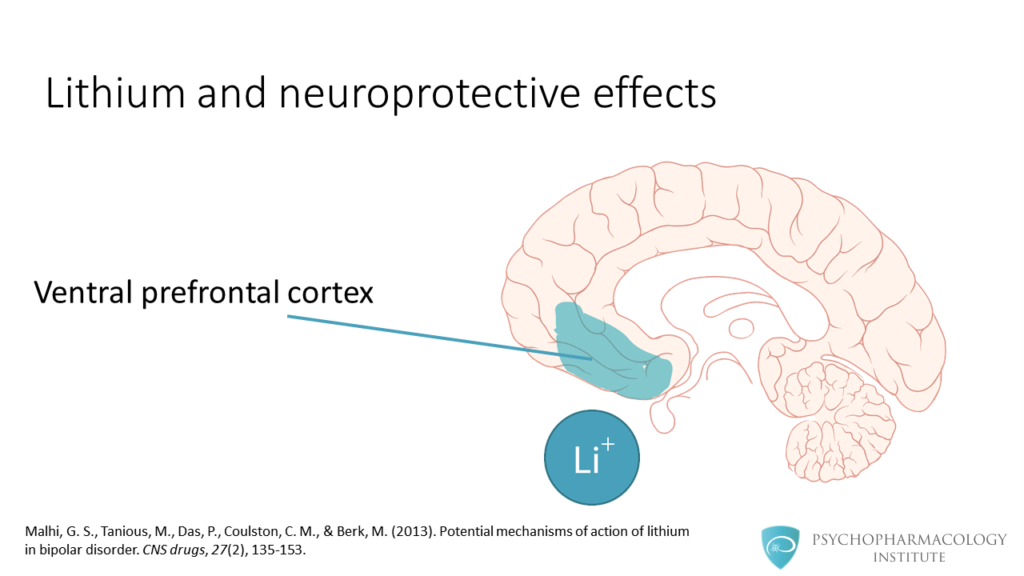
The ventral prefrontal cortex is another brain region linked to lithium neuroprotective effects.

Other regions involved include the hippocampus, paralimbic association cortex and left amygdala.

So, what can we infer from current neuroimaging findings? Probably the key message is that lithium has neuroprotective and neuroproliferative effects, these effects are evidenced by preservation of grey matter. The mechanism of these effects is unknown and the clinical implications are not yet clear.

Let’s continue now with the effects of lithium at the neurotransmission level. As we can see in this slide, lithium modulates neurotransmitters. It inhibits excitatory neurotransmitters such as dopamine and glutamate, and promotes GABA-mediated neurotransmission.
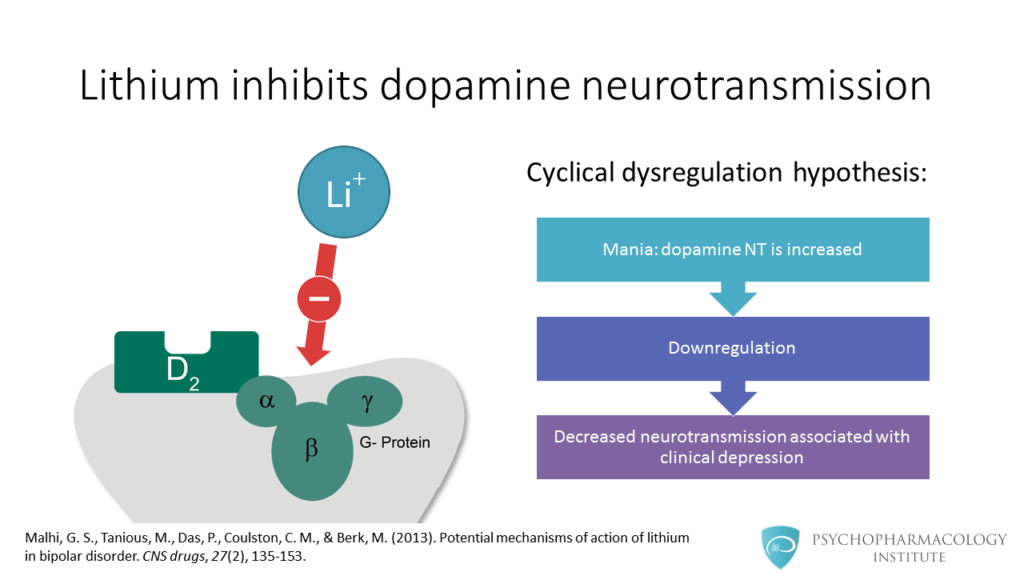
On the left, you can see lithium acting on the dopamine receptor. There is a hypothesis, called the cyclical dysregulation hypothesis. This theory postulates that during mania dopamine neurotransmission is increased. This elevated state would cause downregulation of dopamine receptors. A consequence of downregulation would be decreased dopaminergic neurotransmission associated with clinical depression.
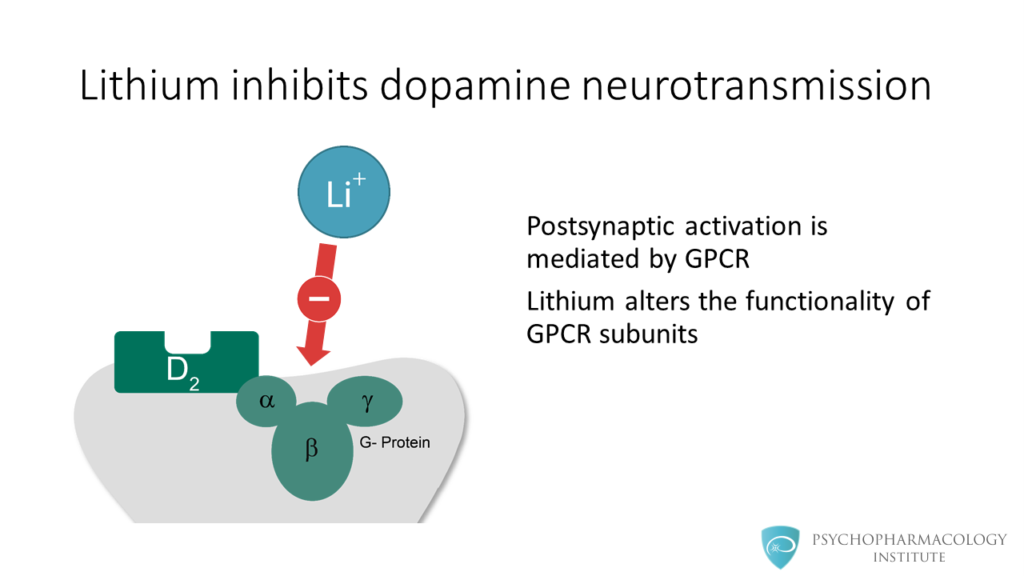
Postsynaptic activation of dopamine receptors is mediated by G-protein coupled receptors or GPCR. Chronic administration of lithium can alter the functionality of GPCR subunits. Because of this, dopaminergic neurotransmission is inhibited.
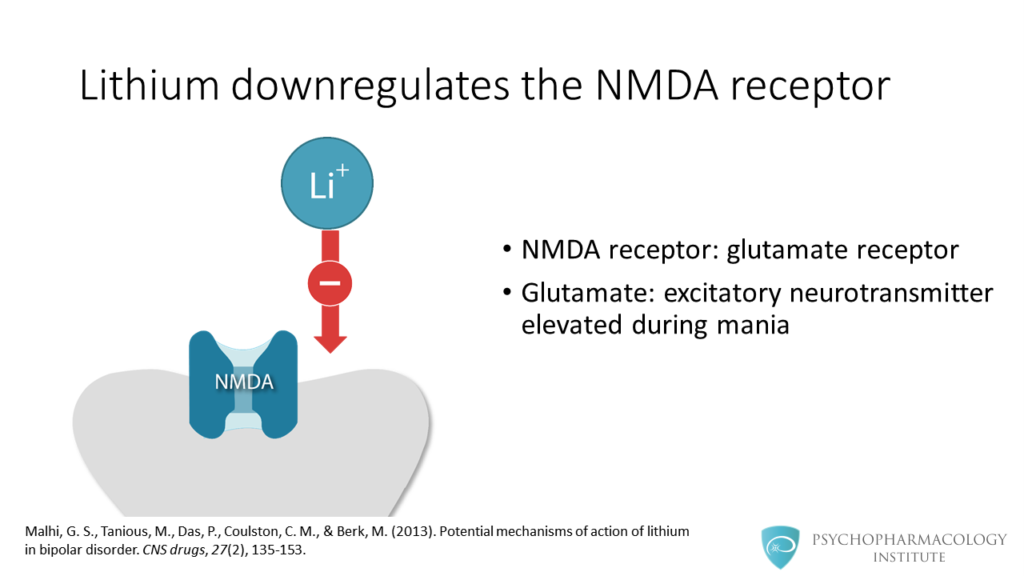
In this slide, we see lithium inducing downregulation of NMDA receptors. As a reminder, the NMDA receptor is a subtype of glutamate receptor. Glutamate is an excitatory neurotransmitter that is elevated during mania.

Lithium acutely stimulates the NMDA receptor, increasing glutamate availability in the postsynaptic neuron. After chronic administration, lithium induces NMDA downregulation, this way lithium modulates glutamate neurotransmission.
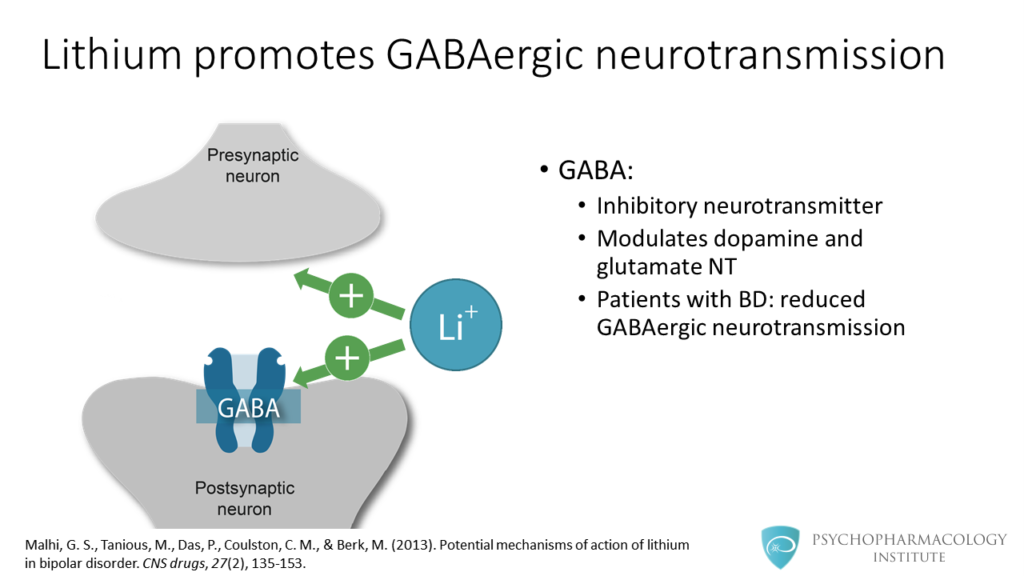
In the previous slides we saw how lithium inhibits excitatory neurotransmission. In this slide we see the effect of lithium on GABAergic neurotransmission. GABA is an inhibitory neurotransmitter that modulates dopamine and glutamate neurotransmission. Research shows that in bipolar patients GABAergic neurotransmission is reduced.
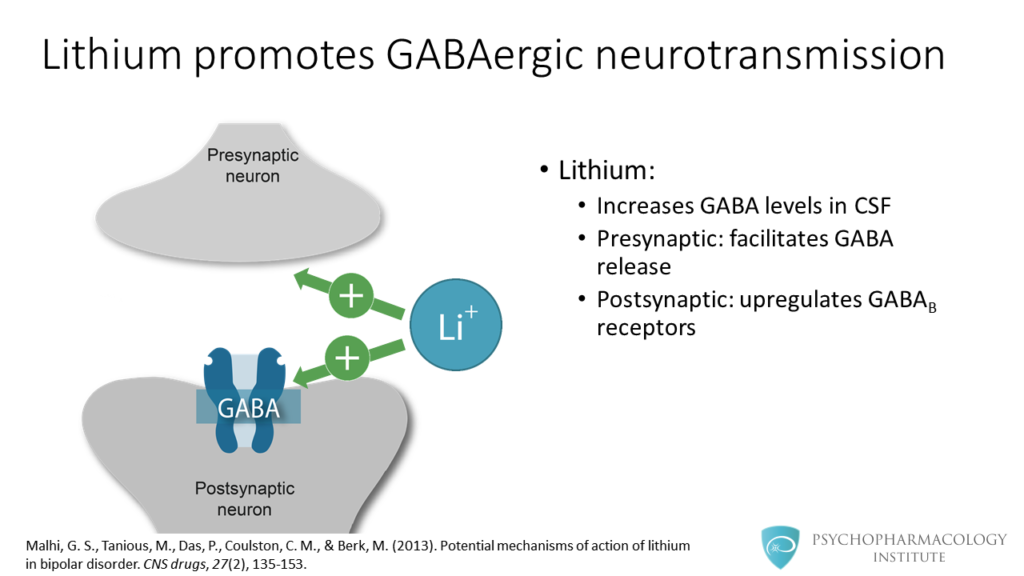
This image shows presynaptic and postsynaptic effects. Lithium increases GABA levels in cerebrospinal fluid. At the presynaptic level, lithium facilitates GABA release. At the postsynaptic level it upregulates GABA-B receptors.
Now we’ll study the potential cellular mechanisms of lithium efficacy. Lithium modulates cellular signaling systems. These systems include adenylate cyclase and cyclic AMP, IMPase, IPPase, Protein Kinase C , GSK-3, BDNF and Bcl – 2.
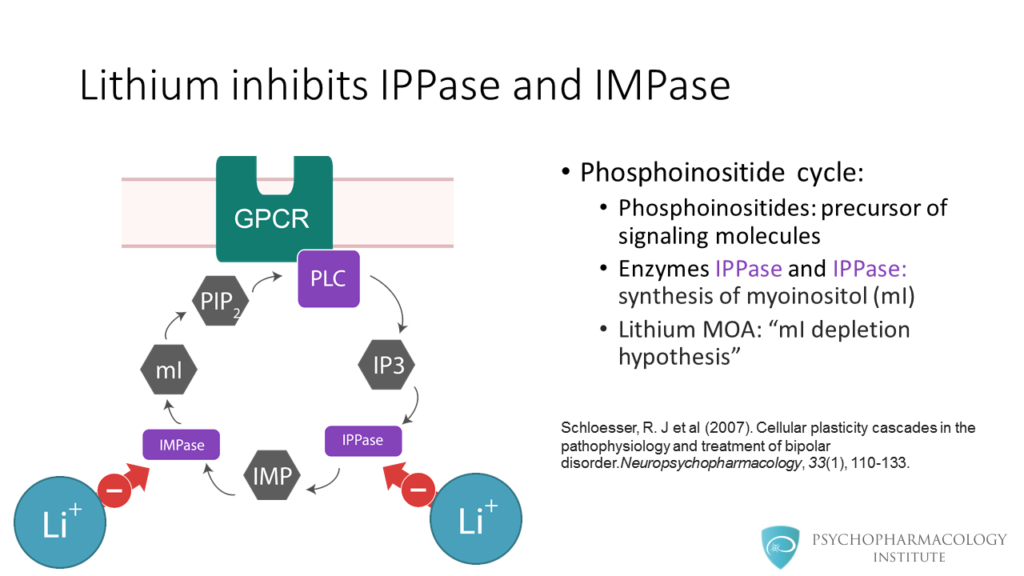
Lithium inhibits IMPase and IPPase. But, what is the context of this? This image shows the phosphoinositide cycle. Phosphoinositides are precursors of signaling molecules. The enzymes shown in purple IPPase and IMPase are involved in the synthesis of myoinositol. Lithium inhibits these two enzymes, and this is the basis for the myinositol depletion hypothesis. Lithium inhibits these enzymes only when they are in excess. There is one caveat though, not all studies have found evidence to support the myinositol depletion hypothesis.
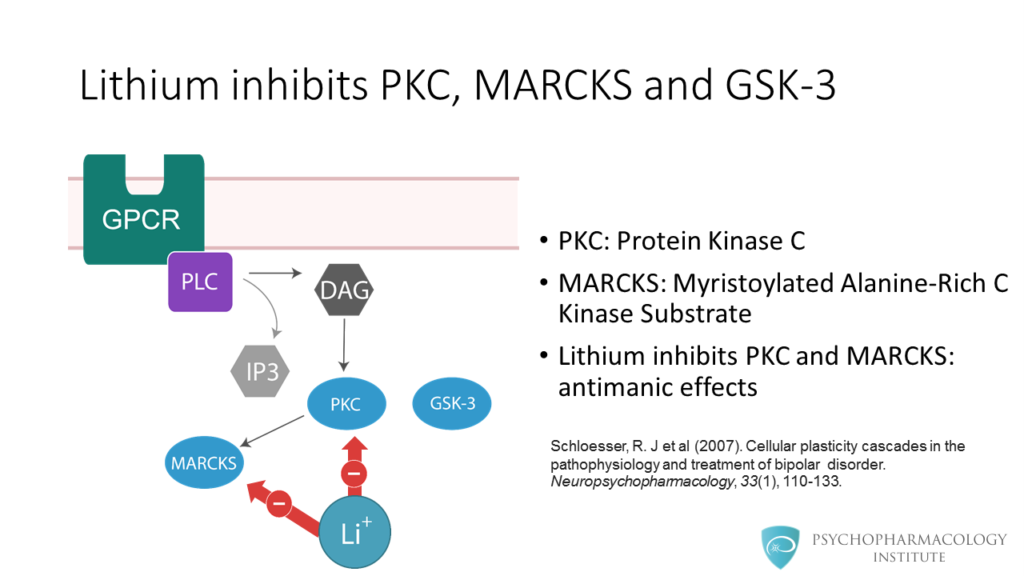
This diagram shows steps after activation of a G-protein coupled receptor. Here in blue we can see Protein Kinase C, MARCKS and GSK-3 in blue. Lithium inhibits PKC and its downstream target MARCKS, this has been linked to antimanic effects.
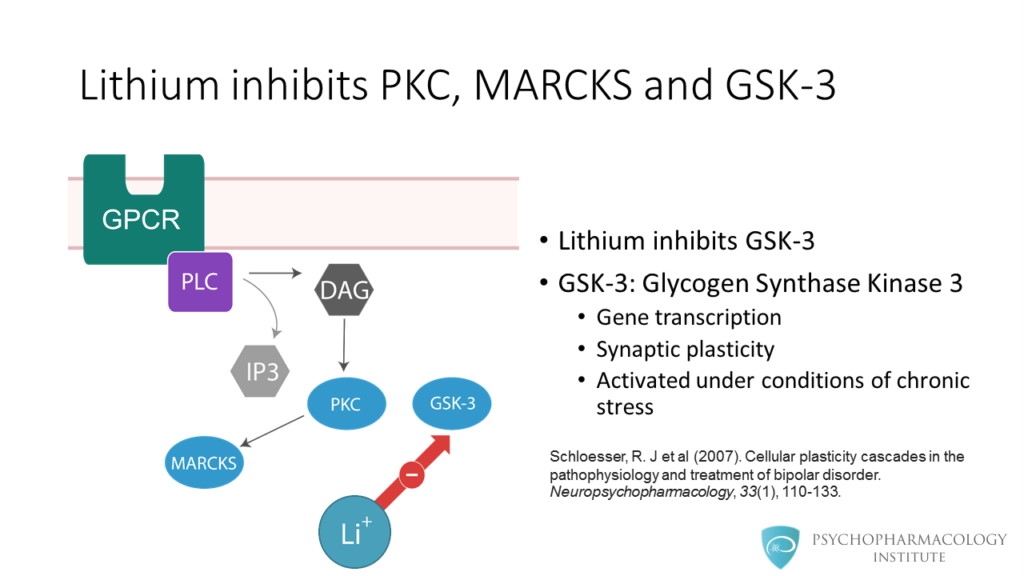
Lithium also inhibits GSK- 3. GSK-3 stands for Glycogen Synthase Kinase 3. This enzyme is involved in gene transcription and synaptic plasticity. In is activated under conditions of chronic stress such as mania.
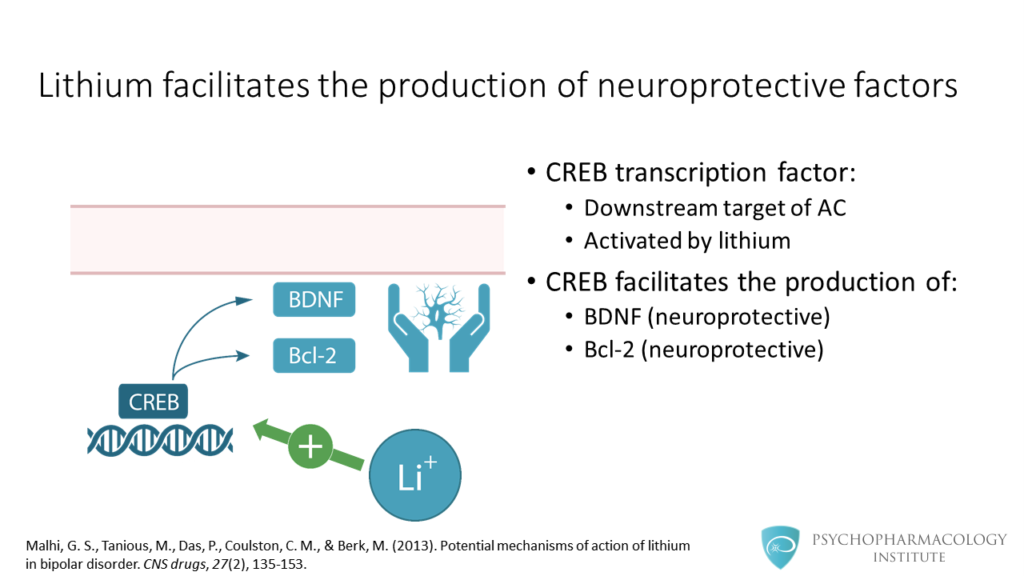
Finally, lithium facilitates the production of neuroprotective factors. CREB transcription factor is a downstream target of adenylyl cyclase and is activated by lithium. The CREB transcription factor facilitates the production of BDNF and Bcl-2, these are neuroprotective factors.
Key Points
The key points are the following:
- Lithium acts on multiple levels, from the macroscopic anatomy to microscopic intracellular signaling.
- Lithium use is associated with a neuroprotective effect, factors such as BDNF and BCL2 have been implicated in this effect.
- There are changes in brain structure associated with lithium use, some of these structures are the anterior cingulate cortex, the ventral prefrontal cortex, the hippocampus and the amygdala.
- At the neurotransmitter level, lihium modulates dopamine, glutamate and GABA neurotransmission.
- At the intracellular signaling level lithium inhibits proteins such as PKC, MARCKS, GSK-3, IPPase and IMPase
References
- Malhi, G. S., Tanious, M., Das, P., Coulston, C. M., & Berk, M. (2013). Potential mechanisms of action of lithium in bipolar disorder . CNS drugs, 27(2), 135-153.
- Schloesser, R. J et al (2007). Cellular plasticity cascades in the pathophysiology and treatment of bipolar disorder .Neuropsychopharmacology, 33(1), 110-133.